You just got your calcium score results back. Maybe the number is zero. Maybe it’s 47. Maybe it’s 312, and now you’re sitting with a printout that feels heavier than it should, wondering what any of it actually means for your heart – and your future.
A coronary calcium score is one of the most revealing numbers in preventive cardiology. It measures the amount of calcified plaque in your coronary arteries, giving doctors – and you – a concrete, quantifiable window into your cardiovascular risk that a standard cholesterol panel simply can’t provide.
The test is called a coronary artery calcium (CAC) scan. It takes less than 10 minutes, requires no dye or needles, and produces a score that has been studied in tens of thousands of patients over decades.
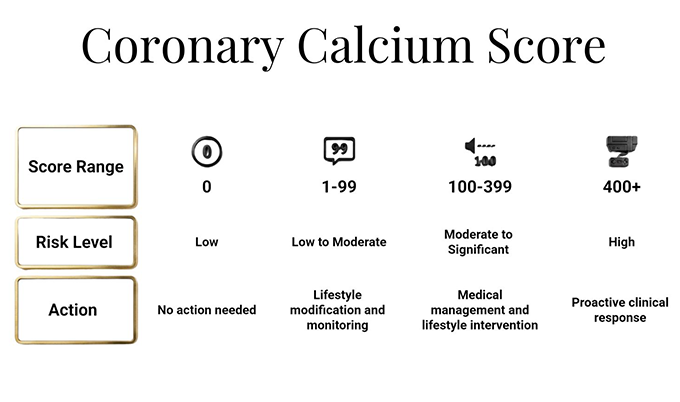
Here’s the short answer on what the numbers mean: a score of zero indicates very low near-term risk. Scores of 1 – 99 suggest mild disease that warrants lifestyle attention. Scores of 100 – 399 indicate moderate plaque buildup. Scores of 400 and above signal extensive calcification and often require immediate medical follow-up.
But the number alone is only part of the story. Where your calcium score results fall relative to others your age and sex, what they mean for your specific risk factors, and what to do next – that’s where the real value lives.
What Is a Coronary Calcium Score, Really?
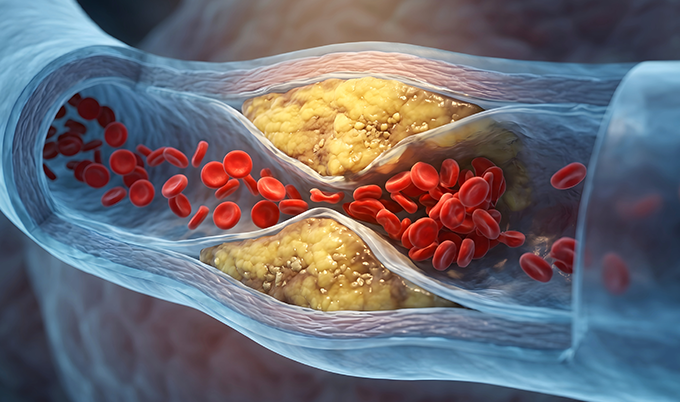
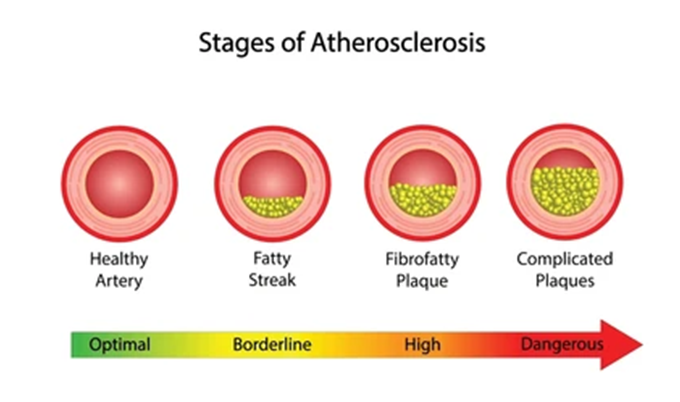
Calcium doesn’t belong in your arteries. When it shows up there, it’s a marker of atherosclerosis – the gradual accumulation of plaque along artery walls that can eventually narrow or block blood flow to the heart.
The calcium itself isn’t the threat. It’s the evidence of a process that started years, sometimes decades, before symptoms ever appear.
A coronary calcium score scan uses a low-dose CT scanner to detect and measure these calcium deposits in the walls of the three major coronary arteries. Each deposit is measured by density and area, and the results are calculated using a formula called the Agatston score – the standard unit you’ll see on your report.
What makes this test so valuable is its specificity. A lipid panel tells you your cholesterol levels. A blood pressure reading tells you about arterial tension. Your calcium score results tell you what has actually happened inside your arteries over time – the biological consequence of those risk factors playing out in your body.
This is why cardiologists increasingly consider the CAC scan one of the most powerful tools available for reclassifying intermediate-risk patients. According to the American Heart Association, the test helps identify who truly needs aggressive treatment versus who can safely hold off – a distinction that standard risk calculators alone often miss.
Coronary Calcium Score Chart: All 4 Ranges Explained
Your report will include a number. That number drops into one of four established categories, each with its own clinical interpretation and recommended action path.
| Calcium Score | Classification | What It Indicates | Typical Next Steps |
|---|---|---|---|
| 0 | No Plaque Detected | No calcified plaque found; very low near-term cardiovascular risk | Maintain healthy lifestyle; may delay statin therapy; rescan in 5 – 7 years if risk factors exist |
| 1 – 99 | Mild Disease | Small amount of plaque present; mildly elevated risk compared to zero | Lifestyle changes (diet, exercise, smoking cessation); discuss statin therapy; rescan in 3 – 5 years |
| 100 – 399 | Moderate Disease | Moderate plaque burden; meaningfully elevated 10-year cardiovascular event risk | Statin therapy typically indicated; aspirin may be considered; aggressive risk factor management |
| 400+ | Extensive Disease | Heavy calcification across coronary arteries; high risk of cardiovascular event | Urgent cardiology evaluation; intensive medical therapy; possible stress testing or additional imaging |
These ranges are consistent across major cardiology guidelines from the American College of Cardiology and the American Heart Association. That said, they’re starting points – not final verdicts.
Your physician will interpret your calcium score results alongside your age, sex, blood pressure, cholesterol levels, smoking history, and family history before drawing any clinical conclusions.
What Is a Good Calcium Score? Why Age and Sex Change Everything
Here’s something that surprises most people: a calcium score of 50 at age 45 carries very different implications than the same score at age 70. The raw number matters. The context matters more.
Cardiovascular risk increases with age. Some degree of arterial calcification is common in older adults – so a score of 80 in a 72-year-old may be relatively unremarkable, while the same score in a 48-year-old raises significant concern because it suggests accelerated arterial aging.
This is why cardiologists use what’s called a percentile ranking – comparing your calcium score results against others of the same age and biological sex. If your score puts you in the 75th percentile for your age group, it means 75% of people your age have less plaque than you do.
General benchmarks by age group tend to follow this pattern:
- Under 45: Any detectable calcium score (above zero) is considered abnormal and warrants discussion with a physician
- Ages 45 – 54: A score of zero is ideal; scores above 100 suggest premature atherosclerosis
- Ages 55 – 64: Some plaque is more common; scores above 300 place a patient in a high-risk category
- Ages 65+: Higher scores are more prevalent; risk stratification depends heavily on percentile ranking and co-existing conditions
Sex-based differences also play a significant role. Women generally develop calcification later than men, so a calcium score of 100 in a 55-year-old woman carries different significance than the same score in a 55-year-old man. The relative risk can actually be higher in women, precisely because the disease typically appears later in their timeline.
Key Insight: There’s no single “good” calcium score that applies to everyone. What matters is where your number falls for your age, sex, and risk profile. A score of 45 may be reassuring at 68 and alarming at 44.
A Calcium Score of Zero – What It Really Means
Yes, a zero score is possible – and it’s the result most people are hoping for. A calcium score of zero means the CT scan found no detectable calcified plaque in your coronary arteries.
That’s genuinely good news. Research consistently shows that a zero score correlates with very low risk of a cardiovascular event over the next 5 to 10 years, according to data published in the Journal of the American College of Cardiology.
But here’s what zero doesn’t mean: it doesn’t mean your arteries are perfectly clean. Non-calcified, “soft” plaque can exist without showing up on a calcium scan.
This is why a zero score is interpreted in context. A 40-year-old with no risk factors can breathe easy. A 45-year-old who smokes, has high blood pressure, and a strong family history of heart disease still has meaningful work to do – the disease process may be underway, just not yet calcified enough to register.
Zero also isn’t permanent. Most guidelines recommend rescanning every 5 – 7 years if you have a zero calcium score but carry risk factors.
What Causes Calcium Score Results to Be High?
No one gets a calcium score of 300 overnight. The plaque that registers on your scan accumulated over years – often decades – driven by a combination of controllable and uncontrollable factors.
The controllable contributors include:
- Smoking: One of the strongest drivers of accelerated atherosclerosis
- High LDL cholesterol: Particularly small, dense LDL particles that penetrate arterial walls
- High blood pressure: Creates shear stress that damages arterial lining and invites plaque formation
- Type 2 diabetes and insulin resistance: Strongly associated with accelerated calcification
- Chronic inflammation: Often diet-driven or linked to conditions like sleep apnea
- Physical inactivity: Absence of cardiovascular exercise allows multiple risk pathways to go unchecked
The uncontrollable contributors include age, biological sex, and family history. If your father had a heart attack at 52, your calcium score results at 48 matter more – and your physician needs that history when interpreting your numbers.
Can You Lower a High Calcium Score?
This is one of the most common questions after receiving results – and the answer is complicated.
You cannot reverse calcified plaque. Once calcium has deposited in an arterial wall, it stays there. That’s why calcium score results only move in one direction: up, or not at all.
What you can do is slow or stop the progression. Research shows that aggressive lifestyle changes and, when appropriate, statin therapy can dramatically reduce the rate at which a calcium score climbs over time.
The goal after receiving a high score isn’t to wish the number away. It’s to take it seriously enough to change the trajectory – from passive worrying to active prevention. That shift is exactly why the scan is worth getting in the first place.
Who Should Get a Calcium Score Test?
The calcium score isn’t for everyone – at least not the same way. The people who benefit most are those in an ambiguous middle zone where standard risk calculators leave questions unanswered.
According to ACC/AHA guidelines, a CAC scan is particularly valuable for:
- Adults aged 40 – 75 with intermediate cardiovascular risk – where calcium score results will meaningfully change the treatment decision
- Patients uncertain about starting statin therapy – a zero score often supports deferring medication; a high score reinforces the case for it
- Adults with a strong family history of early heart disease – especially if other risk markers are borderline
- People with diabetes, metabolic syndrome, or chronic kidney disease who want a clearer picture of their arterial age
- Anyone between 40 and 70 who wants to know their cardiovascular baseline – even without obvious symptoms
The test isn’t designed for people already diagnosed with coronary artery disease, those who have had a prior cardiac event, or anyone on aggressive cardiovascular therapy. For them, the clinical decision has already been made.
Many patients assume they’re too young to worry about coronary calcium. But atherosclerosis doesn’t ask for permission before it begins. Getting a baseline in your mid-40s gives you years of lead time that a first heart attack never would.
✓ Are You a Good Candidate for a Calcium Score Test?
- Between the ages of 40 and 75
- No prior heart attack or coronary artery disease diagnosis
- One or more risk factors: high cholesterol, high blood pressure, smoking, diabetes, or family history
- Intermediate risk on standard cardiovascular risk calculators
- Uncertain about whether to start statin therapy
- Want a concrete, data-driven picture of your cardiovascular health
What Happens During a Calcium Score Scan?
If anxiety about the process is holding you back, it shouldn’t be. The coronary calcium scan is one of the simplest diagnostic tools in preventive cardiology.
Here’s what to expect:
- No preparation required: No fasting, no special diet, no contrast dye injection
- The scan takes under 10 minutes – most of that is positioning, not imaging
- You’ll lie on a CT table while the scanner passes over your chest; you may hold your breath briefly for each image sequence
- There’s no discomfort – the equipment doesn’t touch you during imaging
- Results are reviewed by a board-certified radiologist and typically available within a few days
The radiation exposure from a CAC scan is low – roughly equivalent to a mammogram, and significantly less than a standard diagnostic chest CT.
At Craft Body Scan’s heart scan center, the process is designed to be direct, efficient, and patient-focused – with results reviewed by specialists who understand what your calcium score results mean for your life, not just your chart.
Reading Your Calcium Score Report: What Else Is On It
Beyond the Agatston score, your calcium scan report may include additional information worth understanding.
Per-vessel scores: Your total calcium score is the sum of deposits across all three major coronary arteries – the left anterior descending (LAD), the left circumflex (LCX), and the right coronary artery (RCA). Calcification concentrated in the LAD, which supplies the largest territory of heart muscle, typically receives more clinical attention.
Volume score and mass score: Some reports include these alongside the Agatston score. They’re alternative measurement methods using the same scan data. Your physician will clarify which metric is being used for your risk assessment.
Incidental findings: A calcium scan images a broader section of your chest. Radiologists may note findings unrelated to the coronary arteries – pulmonary nodules, aortic calcification, or other structures that warrant follow-up. These aren’t reasons to panic, but they are reasons to follow up with your doctor.
Your Calcium Score Results Are the Beginning, Not the End
Here’s what matters most after receiving any calcium score: the number is information, not a sentence. A zero doesn’t guarantee you’ll never have a heart attack. A 450 doesn’t mean one is imminent.
What it means is that you now know something about your heart that most people your age don’t – and that knowledge, used well, changes outcomes.
Heart disease kills more Americans than any other condition. It also announces itself more clearly than almost any other disease – if you’re willing to look. Your calcium score results are one of the clearest signals available.
The patients who benefit most from a calcium scan aren’t the ones who get the best scores. They’re the ones who take the results – whatever they are – and do something with them.
Frequently Asked Questions About Calcium Score Results
How often should I repeat a calcium score test?
Most guidelines suggest repeating the scan every 5 – 7 years for patients with a zero score and risk factors, or every 3 – 5 years for those with mild plaque (1 – 99). For scores above 100, your cardiologist will guide the follow-up schedule based on your treatment plan and response to therapy.
Does insurance cover a calcium score scan?
Coverage varies. Some insurance plans cover CAC scans for patients who meet specific risk criteria, but many do not – particularly for asymptomatic screening. Out-of-pocket pricing at Craft Body Scan is structured to make the test accessible without requiring insurance authorization.
Can calcium score results predict a heart attack?
Not precisely. The calcium score measures accumulated plaque – an indicator of long-term cardiovascular risk – rather than predicting an acute event within a specific window. Most heart attacks are caused by the rupture of non-calcified, “soft” plaque, which the CAC scan doesn’t detect. The score is a risk stratification tool, used alongside other clinical information.
Is a calcium score the same as a heart scan?
A coronary calcium score is typically what’s being measured during a heart scan. The terms are often used interchangeably in preventive screening. Some heart scans may include additional imaging components, depending on the facility and the clinical questions being asked.
What’s the difference between a heart scan and a heart and lung scan?
A heart scan focuses on the coronary arteries and calcium scoring. A heart scan and lung scan combines coronary calcium scoring with a low-dose CT of the lungs – screening for both cardiovascular disease and early-stage lung cancer in a single imaging session. For anyone with a smoking history or lung cancer risk factors, the combined scan delivers significantly broader coverage in one appointment.
Know Your Calcium Score Results. Then Act on Them.
A calcium score isn’t a number to file away and forget. It’s one of the most actionable pieces of health information you can have. Whether your result comes back at zero and reinforces everything you’re already doing, or comes back at 280 and changes the conversation with your cardiologist next week – you are better off knowing.
The scan takes less than 10 minutes. The calcium score results it produces can shape 10 years of cardiovascular decisions.
Schedule your heart scan at Craft Body Scan and get the clarity your heart health deserves.