Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult with a qualified healthcare provider regarding any medical condition or treatment plan.
Most women find out they have fibroids the same way. Not because of a scheduled screening. Not because they had a hunch. A fibroid imaging scan ordered for something else - a routine pelvic ultrasound, a whole-body MRI, a CT for abdominal pain - comes back with a line buried in the report: uterine fibroid noted. For many women, that phrase raises more questions than it answers.
Which scan actually found it? Are there more? How big are they? What does any of this mean for your health?
Uterine fibroid imaging includes ultrasound, MRI, CT, and sonohysterography - each modality with different detection capabilities and levels of anatomical detail. Ultrasound is typically the first tool used, while MRI delivers the most complete fibroid imaging available, capturing number, exact location, and size with the highest accuracy. Understanding which type of scan you had, and how to read what your radiologist found, is the first step toward informed decisions about your health.

Uterine Fibroids Are More Common Than Most Women Realize
An estimated 26 million women between the ages of 15 and 50 in the United States have uterine fibroids, according to the National Institutes of Health. By age 49, more than 70% of white women and 84% of Black women have fibroids documented by imaging or surgical records. Lifetime prevalence reaches approximately 75% across all women according to an article published on International Journal of Gynecology & Obstetrics.
Most fibroids cause no symptoms at all. They grow quietly, detected only when a scan captures them incidentally. Of the millions of women who have them, roughly 25 to 30% will experience symptoms significant enough to affect quality of life — heavy bleeding, pelvic pressure, back pain, or bladder and bowel dysfunction.
Fibroids are the leading cause of hysterectomy in the United States, accounting for 39% of all hysterectomies performed annually. That does not mean hysterectomy is inevitable — far from it. But it does highlight why early detection and imaging matter. Knowing your fibroid burden early gives you options that waiting does not.
Why the Type of Fibroid Imaging Scan Changes What You See
Not all fibroid imaging is created equal. A scan that catches one fibroid may miss three others sitting in different locations. A report that says "no fibroids noted" on ultrasound does not always mean the uterus is clear - it may mean the fibroids present were too small or too deeply positioned for that modality to capture.
This matters because treatment planning, surgical preparation, and long-term monitoring all depend on knowing the complete picture - total number, exact location within or around the uterus, and size of each fibroid. Getting an incomplete diagnostic map can lead to incomplete care.
Here is how each imaging method performs, what it can and cannot show, and when each one is appropriate.
Ultrasound Fibroid Imaging: The Standard Starting Point
When a physician suspects fibroids or orders a routine pelvic evaluation, ultrasound is almost always the first fibroid imaging tool used. It is accessible, relatively inexpensive, and does not involve radiation. Two types are commonly performed.
Transabdominal ultrasound uses a handheld probe moved across the surface of the abdomen. It gives a broad view of the uterus and surrounding structures, working well for larger fibroids that are clearly visible from the outside.
Transvaginal ultrasound (TVUS) uses a smaller probe inserted internally, placing the transducer much closer to the uterus for sharper images. According to the American Academy of Family Physicians, transvaginal ultrasound is approximately 90 to 99% sensitive for uterine fibroid detection in most cases.
The limitation of ultrasound fibroid imaging? It can miss subserosal fibroids on the outer surface of the uterus, and smaller lesions can fall below detection thresholds. It is also operator-dependent - the experience of the sonographer affects what gets captured. A 2025 review in the International Journal of Gynecology and Obstetrics found that only 23% of ultrasound reports met all quality criteria recommended by international guidelines.
When ultrasound findings are unclear, fibroids are multiple, or surgical planning is needed, MRI becomes the recommended next step.
| Imaging Type | Sensitivity | Best For | Limitation |
|---|---|---|---|
| Transvaginal Ultrasound | 90–99% | First-line screening | May miss small or subserosal fibroids |
| MRI | 98.9% | Complete fibroid mapping, surgical planning | Higher cost; limited access in some areas |
| CT Scan | Moderate (calcified) | Incidental detection; calcified fibroids | Radiation; poor soft tissue contrast |
| Sonohysterography | High (cavity) | Submucosal fibroids; uterine cavity detail | Invasive; not used for initial screening |
MRI Fibroid Imaging: The Most Complete Picture Available
MRI is the gold standard for fibroid imaging. It does not use radiation. It produces detailed, multi-plane images of soft tissue that ultrasound simply cannot match - particularly for fibroids that are small, deeply embedded, or located in challenging anatomical positions.
A 2024 cross-sectional study found MRI fibroid imaging achieved a sensitivity of 98.9% and specificity of 97.1%, compared to 88.2% sensitivity and 85.7% specificity for ultrasound. MRI identified an average of 3.1 fibroids per patient versus 2.3 by ultrasound - a meaningful gap when treatment depends on knowing the full count.
Earlier research from the National Institutes of Health showed MRI sensitivity was approximately double that of ultrasound against pathological specimens. Even after excluding fibroids under 1 cm, ultrasound sensitivity remained low at 47% - while MRI continued to outperform.
MRI is particularly valuable in three clinical situations:
- Preoperative surgical planning - Surgeons need to know exactly how many fibroids are present, where each sits, and what adjacent structures are involved before myomectomy or other procedures.
- Distinguishing fibroids from other conditions - Adenomyosis and uterine sarcoma can look similar to fibroids on ultrasound. MRI provides tissue contrast that differentiates these conditions with far greater accuracy.
- Monitoring treatment response - For women undergoing uterine artery embolization or MRI-guided focused ultrasound, repeat imaging tracks whether fibroids have responded as expected.
Whole-body MRI, the kind available at Craft Body Scan, captures the uterus as part of a head-to-pelvis evaluation. Fibroids are regularly identified during these scans - not because the woman suspected anything, but because fibroid imaging covered the full pelvic region. That incidental discovery, when caught early and characterized clearly, leaves far more treatment options available.
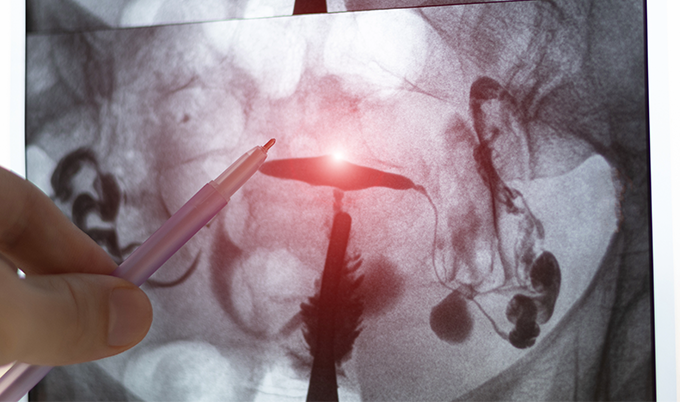
CT Scan Fibroid Imaging: The Incidental Finder
CT scanning is not a first-choice tool for fibroid imaging - it lacks MRI's soft tissue detail and involves ionizing radiation. What CT does capture, particularly during full body screening, are calcified fibroids and larger uterine masses discovered incidentally. Calcified fibroids appear as dense, clearly demarcated structures on CT. For younger women with non-calcified fibroids, CT detection is less reliable.
When a CT report flags a uterine mass, the follow-up is almost always ultrasound or MRI. CT is a starting point, not a complete diagnostic answer. See what a full body CT scan captures across all major organs.
Sonohysterography: Fibroid Imaging Inside the Uterine Cavity
Sonohysterography, also called saline infusion sonography (SIS), combines ultrasound with sterile saline injected into the uterine cavity. The fluid creates contrast that makes the interior of the uterus visible in detail - particularly useful for fibroid imaging of lesions that grow into or distort the uterine cavity.
These are called submucosal fibroids, and they are the type most closely linked to abnormal bleeding and fertility problems. Standard ultrasound can miss them or underestimate cavity involvement. Sonohysterography resolves that ambiguity with considerably more accuracy.
It is typically used when a woman has unexplained heavy bleeding, recurrent miscarriage, or difficulty conceiving, and standard ultrasound fibroid imaging has not provided a clear enough answer.
Reading Your Fibroid Imaging Report: What the Terms Actually Mean
Fibroid imaging reports use specific clinical language that can feel impenetrable. Breaking it down makes the findings far less intimidating.
Location categories in any fibroid imaging report describe where the fibroid sits relative to the uterine wall:
- Submucosal - Growing into or toward the uterine cavity. Most likely to cause heavy bleeding and affect fertility. Even small submucosal fibroids carry significant clinical impact.
- Intramural - Within the muscular wall of the uterus. The most common type identified in fibroid imaging. Symptoms depend on size.
- Subserosal - Growing outward from the uterus toward the outer surface. Often causes bulk symptoms - pressure, back pain, urinary frequency - rather than bleeding.
- Pedunculated - Attached to the uterus by a stalk. Can originate from submucosal or subserosal positions.
The FIGO classification system assigns fibroids a number from 0 to 8 based on their exact position. Type 0 fibroids are entirely within the uterine cavity with no intramural component. Type 8 fibroids have no attachment to the myometrium at all. Types in between describe varying degrees of cavity involvement and wall penetration. When your radiologist references a FIGO type in a fibroid imaging report, they are providing a standardized position map that directly shapes treatment decisions.
Size measurements are reported in centimeters across three dimensions. A 2.3 x 1.8 x 1.9 cm fibroid is small and typically warrants only monitoring. A 7 cm fibroid exerting pressure on the bladder wall is a different clinical picture entirely.
"Heterogeneous signal" or "calcification" in fibroid imaging describes internal characteristics - whether the tissue is consistent throughout or contains areas of degeneration. Most degenerating fibroids are benign, but these imaging signal patterns help radiologists flag cases where further assessment is warranted.
What to Ask After Receiving Fibroid Imaging Results
- How many fibroids were identified, and where is each located?
- What is the FIGO classification for each fibroid found?
- Are any fibroids submucosal - near or inside the cavity?
- Do my imaging findings explain my current symptoms?
- Would a follow-up MRI provide more complete fibroid imaging?
- How often should I repeat fibroid imaging to monitor changes?
Take Action on Your Fibroid Imaging Results
A fibroid finding on imaging is not a diagnosis requiring immediate treatment. Most fibroids are monitored rather than removed. But knowing what you have - accurately and completely - determines every decision that follows.
If your ultrasound shows one small intramural fibroid with no symptoms, watchful waiting with periodic fibroid imaging checks is typically appropriate. If MRI reveals five fibroids including two submucosal lesions alongside heavy bleeding, a different specialist conversation begins. The fibroid imaging report does not make the decision. It gives you the information to make it yourself, with your doctor, based on the full clinical picture.
For women in their 30s and 40s - when fibroids are most actively growing - a whole-body scan provides baseline fibroid imaging that routine visits rarely capture. Fibroids found before they become symptomatic leave far more treatment options available. Explore related screening through our cancer screening page and whole-body MRI overview.
At Craft Body Scan, whole-body MRI evaluations include detailed pelvic imaging reviewed by board-certified radiologists. If a fibroid is present, you will know its location, classification, and what it means for your health.
Ready to get a clear picture of what is happening inside your body? Schedule your scan today and take the first step toward early detection and answers that help you move forward.