Every minute counts during a stroke. When brain cells lose their blood supply, they die at an alarming rate – approximately 1.9 million neurons every 60 seconds. A stroke brain scan is the only way to determine what type of stroke you’re experiencing and whether you’re a candidate for life-saving treatment within the critical 3-4.5 hour window.
The brain imaging happens within minutes of arriving at the emergency department. CT scans take seconds to complete. MRI sequences finish in 10-15 minutes.
These rapid stroke brain scan protocols determine whether doctors can administer clot-busting medications. Understanding early warning signs helps you recognize when someone needs emergency stroke imaging immediately.
The faster you identify symptoms using the FAST acronym, the faster treatment begins. Better treatment timing creates better recovery outcomes after brain scan confirms the diagnosis.
Understanding Why Stroke Brain Scans Are Time-Critical Medical Emergencies

Stroke is the fifth leading cause of death in the United States. Approximately 800,000 Americans experience stroke annually according to 2025 Heart Disease and Stroke Statistics from the American Heart Association.
Brain tissue cannot survive without oxygen carried by blood flowing to neurons. When that blood supply stops – whether from a clot or bleeding – cells begin dying immediately without intervention.
Doctors describe this urgency as “time is brain” when discussing stroke brain scan protocols. Research shows middle cerebral artery occlusion destroys 9 million neurons per minute during untreated stroke.
That’s 540 million neurons lost every hour without treatment. Each lost neuron means potential permanent disability affecting movement, speech, or cognition after stroke occurs.
A brain scan reveals whether the stroke is ischemic (caused by a blocked blood vessel) or hemorrhagic (caused by bleeding). This distinction is absolutely critical because treatments differ completely between stroke types requiring different emergency interventions.
Thrombolytic therapy dissolves clots in ischemic strokes diagnosed on stroke brain scan. But giving clot-busting drugs to someone with bleeding detected on imaging would be fatal to that patient.
The stroke brain scan provides the answer within minutes of emergency department arrival.
 Why Immediate Stroke Brain Scan Matters
Why Immediate Stroke Brain Scan Matters
- 1.9 million neurons die every minute without treatment
- 3-4.5 hour window for clot-busting medication administration
- Distinguishes stroke types requiring completely different treatments
- Guides surgical decisions for mechanical clot removal procedures
- Identifies salvageable tissue that can be saved with rapid intervention
- Predicts recovery outcomes based on infarct size and location
- Prevents fatal errors like giving blood thinners to hemorrhage patients
Recognizing Early Warning Signs Requiring Immediate Stroke Brain Scan
The American Stroke Association promotes the FAST acronym to help people identify stroke symptoms quickly. Recent 2025 research presented at the International Stroke Conference confirms both FAST and BE FAST acronyms effectively motivate people to call 911 immediately for suspected stroke requiring stroke brain scan evaluation.
Face drooping: Ask the person to smile. One side of the face may droop or feel numb creating an uneven appearance.
The smile appears lopsided on one side. Facial numbness accompanies drooping in most stroke cases requiring emergency stroke brain scan.
Arm weakness: Ask the person to raise both arms above their head. One arm may drift downward involuntarily or feel weak and numb throughout.
The affected arm cannot maintain elevation. This unilateral weakness indicates brain damage visible on stroke brain scan imaging studies.
Speech difficulty: Ask the person to repeat a simple sentence like “The sky is blue today.” Speech may be slurred, incomprehensible, or completely absent despite effort.
Some patients cannot speak at all. Others produce garbled sounds without recognizable words when stroke affects language centers revealed on stroke brain scan.
Time to call 911: If you observe any of these signs, call emergency services immediately without delay. Don’t drive to the hospital yourself or wait to see if symptoms improve on their own.
The expanded BE FAST acronym adds two crucial warning signs before the traditional FAST symptoms:
Balance loss: Sudden trouble with balance or coordination that makes walking difficult or impossible. The person may stumble, fall, or cannot walk straight lines requiring stroke brain scan evaluation.
Eyes affected: Sudden blurred vision, double vision, or loss of vision in one or both eyes without pain. Visual disturbances appear suddenly rather than gradually developing over time before stroke brain scan.
These symptoms appear suddenly rather than developing gradually. That sudden onset distinguishes stroke from other conditions that develop slowly over days or weeks.
Some people experience all symptoms together. Others show only one or two warning signs initially. Any combination requires immediate emergency response and stroke brain scan evaluation without delay.
 When to Call 911 for Stroke Brain Scan
When to Call 911 for Stroke Brain Scan
- Sudden facial drooping on one side when asked to smile
- Arm drift or weakness when both arms raised simultaneously
- Slurred or absent speech when repeating simple sentences
- Loss of balance or sudden coordination problems walking
- Vision changes including blurred, double, or complete vision loss
- Severe sudden headache unlike any previous headache experienced
- Confusion or trouble understanding what others are saying
- Any symptom resolving – TIA still requires emergency evaluation
Types of Stroke Brain Scans Used in Emergency Departments
Emergency departments use two primary imaging technologies for acute stroke diagnosis requiring rapid stroke brain scan completion. The choice depends on availability, patient condition, and clinical urgency factors.
Non-Contrast CT Stroke Brain Scan
CT (computed tomography) remains the most common initial stroke brain scan performed in emergency departments. The entire head scan completes in seconds making it ideal for time-critical stroke evaluation.
Most emergency departments have CT scanners available 24/7 for immediate stroke brain scan studies. The non-contrast CT excels at detecting bleeding in the brain tissue.
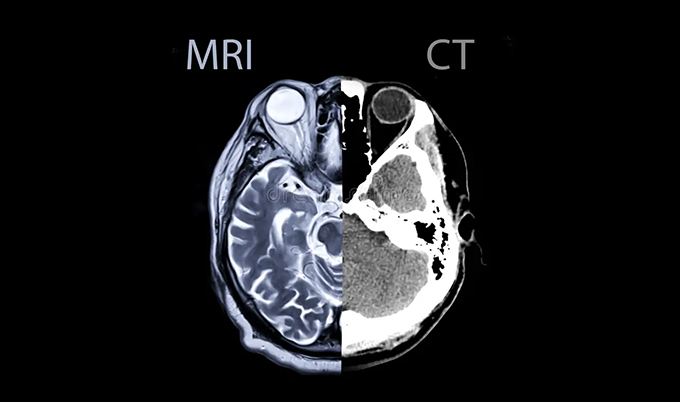
Hemorrhagic strokes appear bright white on CT images immediately after bleeding occurs. This allows doctors to rule out bleeding before considering clot-busting medications that would worsen hemorrhage.
However, CT sensitivity for detecting ischemic stroke is only 40-60% in the first six hours after symptom onset. Early ischemic changes appear subtle on initial stroke brain scan CT images.
Brain tissue doesn’t show obvious damage for several hours after blood flow stops. Radiologists look for specific early CT signs of stroke on initial stroke brain scan:
– Loss of grey-white matter differentiation in affected areas
– Subtle brain swelling in regions experiencing ischemia
– Hyperdense (bright) middle cerebral artery indicating clot location
– Insular ribbon sign showing early cortical infarction patterns
The Alberta Stroke Program Early CT Score (ASPECTS) quantifies early stroke changes visible on stroke brain scan CT imaging. Radiologists score ten brain regions supplied by the middle cerebral artery circulation.
Each affected region loses one point from a perfect score of 10. Lower ASPECTS scores predict worse outcomes and higher hemorrhage risk with treatment.
CT Angiography Stroke Brain Scan
CT angiography immediately follows the non-contrast scan in most stroke brain scan protocols. Technicians inject iodinated contrast through an IV line placed in your arm.
Rapid imaging captures contrast flowing through brain arteries. CTA identifies large vessel occlusions requiring mechanical thrombectomy procedures for clot removal.
The imaging shows exactly which artery is blocked and where the clot is located. This guides interventional neuroradiologists during emergency stroke brain scan-directed clot removal procedures.
CTA sensitivity and specificity approach 100% for detecting intracranial vessel occlusions. The 3D reconstructions help surgeons plan their approach for endovascular procedures removing blood clots.
CT Perfusion Stroke Brain Scan
CT perfusion measures blood flow through brain tissue as part of comprehensive stroke brain scan protocols. Rapid sequential imaging tracks contrast moving through different vascular territories in your brain.
Computer analysis calculates critical parameters:
Cerebral blood flow (CBF) – How much blood reaches each brain region per minute
Cerebral blood volume (CBV) – Total blood present in tissue at any moment
Mean transit time (MTT) – How long blood takes to pass through vessels
This stroke brain scan information distinguishes dead tissue (infarct core) from salvageable tissue (penumbra). The ischemic penumbra represents brain tissue at risk but still viable with rapid treatment.
Rapid reperfusion can save penumbral tissue identified on stroke brain scan perfusion studies. CT perfusion helps select patients for thrombectomy even beyond traditional 4.5-hour time windows.
Some people with large penumbras benefit from intervention 6-24 hours after symptom onset. Advanced stroke brain scan perfusion imaging identifies these extended-window treatment candidates.
| Stroke Brain Scan Type | Scan Duration | Primary Purpose | Sensitivity for Acute Stroke |
|---|---|---|---|
| Non-Contrast CT | 30-60 seconds | Exclude hemorrhage, detect early ischemia | 40-60% in first 6 hours |
| CT Angiography | 2-3 minutes | Identify vessel occlusions | Up to 100% for large vessels |
| CT Perfusion | 5-7 minutes | Measure tissue viability | 73% with perfusion added |
| MRI DWI | 10-15 minutes | Detect early ischemic changes | Over 95% from onset |
MRI Stroke Brain Scan with Diffusion-Weighted Imaging
MRI provides superior sensitivity for detecting acute ischemic stroke compared to CT scanning. Diffusion-weighted imaging detects ischemic changes within minutes of stroke onset on stroke brain scan MRI studies.
DWI measures water molecule movement between brain cells affected by ischemia. Normal healthy neurons allow free water movement throughout cellular structures.
During acute stroke visible on stroke brain scan, intracellular injury traps water inside dying cells. Restricted water diffusion appears bright white on DWI images revealing stroke location immediately.
This signal change occurs within 3-30 minutes of blood flow cessation. DWI improves stroke detection from 50% to over 95% compared to CT alone when performing stroke brain scan evaluation.
Apparent diffusion coefficient (ADC) maps confirm acute infarction. Areas that are bright on DWI and dark on ADC represent true acute stroke rather than other causes of restricted diffusion visible on stroke brain scan.
MRI multimodal stroke brain scan protocols include:
– T1-weighted images for anatomical detail and tissue characterization
– T2-weighted images for subacute changes developing over hours
– FLAIR sequences to detect subtle edema and subarachnoid hemorrhage
– Gradient echo sequences sensitive to blood products and prior hemorrhage
– MR angiography to visualize vessel occlusions without contrast injection
– Perfusion imaging to identify salvageable penumbra requiring urgent treatment
The main limitation of MRI for acute stroke brain scan is availability. Not all hospitals have MRI machines in or near the emergency department for immediate imaging.
MRI also takes longer than CT – typically 15-30 minutes for complete stroke brain scan stroke protocol sequences. Certain patients cannot undergo MRI due to implanted devices contraindicating magnetic fields.
Pacemakers, cochlear implants, and some orthopedic hardware contraindicate MRI completely. CT becomes the only option for these patients requiring emergency stroke brain scan evaluation.
How Stroke Brain Scans Guide Emergency Treatment Decisions
The stroke brain scan determines your treatment pathway within minutes of completing imaging. Radiologists interpret scans immediately and communicate findings to the emergency medicine team waiting for results.
Thrombolytic Therapy Window After Stroke Brain Scan
Tissue plasminogen activator (tPA) dissolves blood clots causing ischemic strokes. This clot-busting medication must be administered within 3-4.5 hours of symptom onset for FDA approval after stroke brain scan confirms eligibility.
The stroke brain scan must show:
– No evidence of intracranial hemorrhage anywhere in brain tissue
– No large established infarction (greater than one-third middle cerebral artery territory)
– No other contraindications to thrombolysis identified on imaging
CT imaging excludes hemorrhage effectively before thrombolytic therapy. Even subtle bleeding contraindicates tPA administration entirely.
The consequences of giving clot-busters to someone bleeding in their brain detected on stroke brain scan would be catastrophic and potentially fatal to that patient.
MRI provides additional information through diffusion-perfusion mismatch patterns. Large mismatch indicates substantial penumbra – salvageable tissue that could benefit from reperfusion therapy guided by stroke brain scan findings.
Mechanical Thrombectomy Selection Using Stroke Brain Scan
Large vessel occlusions often require mechanical clot removal rather than just medication. Interventional neuroradiologists thread catheters through arteries to the brain guided by stroke brain scan imaging.
Specialized devices capture and extract the clot directly. The stroke brain scan determines thrombectomy candidacy through multiple factors:
– CTA confirms large vessel occlusion location and clot characteristics
– Perfusion imaging quantifies salvageable tissue volume remaining
– Collateral circulation assessment predicts procedure success likelihood
Recent trials extended thrombectomy windows to 6-24 hours for selected patients. Imaging-based selection using advanced stroke brain scan protocols identifies people with favorable perfusion profiles despite late presentation.
Hemorrhagic Stroke Management Guided by Stroke Brain Scan
Hemorrhagic strokes require completely different management than ischemic strokes. The stroke brain scan guides surgical decision-making for bleeding control and pressure reduction.
CT immediately identifies critical information:
– Intracerebral hemorrhage location and total volume
– Intraventricular hemorrhage extension into ventricles
– Hydrocephalus from blocked CSF circulation pathways
– Mass effect and midline shift indicating dangerous pressure
Large hemorrhages causing significant mass effect may require surgical evacuation. Neurosurgeons remove blood clots compressing critical brain structures based on stroke brain scan findings.
The stroke brain scan determines surgical urgency and approach. CTA can identify underlying aneurysms or arteriovenous malformations causing the bleeding requiring repair.
These vascular abnormalities require intervention to prevent rebleeding. Follow-up stroke brain scan imaging monitors for rebleeding complications.
What to Expect During Your Emergency Stroke Brain Scan

Understanding the stroke brain scan process reduces anxiety during this terrifying medical emergency. Here’s what typically happens from ambulance arrival through imaging completion.
Emergency Department Arrival for Stroke Brain Scan
Paramedics alert the hospital before arrival when they suspect stroke. This activates the stroke team ready to perform immediate stroke brain scan evaluation.
Neurologists, radiologists, and specialized nurses assemble immediately. You’ll go directly to the CT scanner – usually within 10-15 minutes of arrival for stroke brain scan.
Some advanced stroke centers have CT scanners inside the emergency department. This eliminates transport time before stroke brain scan completion.
The entire stroke brain scan protocol including non-contrast CT, CTA, and perfusion takes about 5-10 minutes total. You lie flat on the CT table for scanning.
The scanner makes clicking and whirring sounds during image acquisition. The table moves through the doughnut-shaped scanner opening automatically.
Your head remains still inside a foam holder preventing movement. The actual scanning takes only seconds for non-contrast CT portion of stroke brain scan.
For CTA, technicians inject iodinated contrast through an IV line. You may feel warmth spreading through your body during contrast injection.
Some people report a metallic taste temporarily. These sensations are normal and resolve quickly after stroke brain scan completion.
If MRI Stroke Brain Scan Is Performed
Some hospitals use MRI as first-line stroke brain scan instead of CT. Emergency MRI requires specialized protocols optimized for speed without sacrificing diagnostic quality.
Rapid stroke MRI protocols complete in 10-15 minutes total. This includes diffusion imaging, FLAIR, gradient echo, and MR angiography sequences for comprehensive stroke brain scan.
You’ll lie on a narrow table that slides into the MRI tunnel. The scanner is louder than CT – making loud banging and buzzing noises during stroke brain scan acquisition.
Technicians provide earplugs or headphones protecting your hearing. Absolute stillness is critical for image quality throughout the stroke brain scan procedure.
Even small movements blur the images requiring sequence repeats. Technicians may position foam padding around your head preventing any motion.
Immediate Results Communication After Stroke Brain Scan
Radiologists interpret stroke brain scan results immediately without delay. Results reach the emergency team within minutes of imaging completion.
Time-critical decisions cannot wait for formal written reports. If you’re a candidate for tPA based on stroke brain scan findings, doctors begin treatment immediately without hesitation.
The medication infuses through IV over 60 minutes. You’ll have continuous monitoring for complications during infusion.
For large vessel occlusions requiring thrombectomy identified on stroke brain scan, the interventional team prepares immediately. Transfer to the angiography suite happens within minutes of imaging confirmation.
Silent Strokes and Follow-Up Stroke Brain Scans
Some people experience strokes without obvious symptoms detected at the time. These “silent strokes” often go undetected until incidental imaging years later reveals old infarcts on routine stroke brain scan studies.
Silent strokes appear as small white spots on MRI scans. The affected brain regions were presumably non-eloquent areas not controlling critical functions during stroke brain scan evaluation.
Symptoms were too subtle to notice consciously. Or they were attributed to other causes rather than recognized as stroke requiring emergency stroke brain scan at the time.
Research shows silent strokes are surprisingly common in certain populations. They increase risk for future symptomatic strokes requiring emergency treatment.
They also contribute to cognitive decline over time. If you’re at high risk for stroke, preventive stroke brain scan imaging may identify silent infarcts or other concerning changes.
Risk factors include:
– Uncontrolled high blood pressure over many years
– Atrial fibrillation causing irregular heart rhythm
– Diabetes affecting blood vessel health throughout body
– Prior TIA or stroke history increasing recurrence risk
– Strong family history of stroke in multiple relatives
Stroke Prevention and Risk Factor Screening Using Brain Scans
While emergency stroke brain scan imaging focuses on acute diagnosis, specialized imaging helps prevent first or recurrent strokes. Carotid artery ultrasound detects atherosclerotic plaque buildup narrowing arteries.
Significant carotid stenosis increases stroke risk dramatically. Identifying high-grade narrowing allows surgical intervention before stroke occurs requiring emergency stroke brain scan.
MRI can assess blood vessel health and plaque stability. Advanced sequences detect vulnerable plaques likely to rupture causing stroke.
This allows doctors to start preventive medications aggressively. Cardiac imaging identifies embolic sources sending clots to the brain requiring stroke brain scan evaluation.
Echocardiography reveals clots in heart chambers detectable on imaging. It also shows valve abnormalities and structural defects creating stroke risk.
Brain MRI in stroke survivors guides secondary prevention strategies. Imaging patterns visible on stroke brain scan studies suggest specific stroke mechanisms:
– Multiple small vessel infarcts suggest hypertensive small vessel disease
– Watershed infarcts suggest low flow states or cardiac issues
– Embolic pattern suggests cardiac or large vessel source
Cost Considerations for Emergency Stroke Brain Scans
Emergency stroke brain scan imaging is always considered medically necessary during suspected stroke. Insurance typically covers imaging without prior authorization when stroke is suspected clinically.
Out-of-pocket costs depend on your insurance plan deductibles and copays. Emergency CT brain scans cost $500-$3,000 without insurance coverage.
Adding CTA and perfusion increases total costs to $2,000-$8,000 for complete stroke brain scan protocol. MRI stroke protocols cost $800-$6,000 without insurance depending on facility.
The higher cost reflects longer scan time and technical complexity. Most insurance plans cover emergency stroke care at in-network rates even when you go to out-of-network hospitals for stroke brain scan.
Federal law requires stabilizing treatment regardless of insurance status. Never delay calling 911 due to cost concerns about stroke brain scan expenses.
Stroke treatment is time-critical for optimal outcomes. Financial counselors can help with billing after your medical emergency is stabilized following stroke brain scan.
When to Seek Preventive Stroke Brain Scan Evaluation
If you’re experiencing warning signs like temporary vision loss, brief weakness, or transient speech difficulty, don’t wait for symptoms to worsen. These could be transient ischemic attacks (TIAs) – “warning strokes” that resolve spontaneously but require stroke brain scan evaluation.
TIAs indicate high risk for full stroke within days. About 30% of people experiencing TIA have a major stroke within three months without intervention discovered through stroke brain scan imaging.
Immediate evaluation with stroke brain scan is crucial. Seek emergency evaluation for these symptoms:
– Any sudden neurological symptoms even if they resolve completely
– First-time severe headache unlike any previous headache experienced
– Sudden confusion or trouble understanding speech from others
– Sudden numbness or weakness anywhere in your body
– Sudden difficulty walking or loss of coordination
Don’t adopt a “wait and see” approach with neurological symptoms. The window for beneficial intervention discovered through stroke brain scan is measured in hours, not days or weeks.
According to research from the National Institutes of Health, early intervention within the first hours after symptom onset provides the best chance for complete recovery. At Craft Body Scan, we understand the critical importance of early detection for serious health conditions.
While our focus is on preventive health screening for asymptomatic individuals, we recognize that stroke requires immediate emergency evaluation. Our board-certified radiologists emphasize that suspected stroke symptoms always warrant calling 911 rather than scheduling elective imaging studies.
The American Heart Association provides comprehensive guidelines on stroke diagnosis and treatment protocols. These guidelines emphasize that every minute of delay increases permanent disability risk.
Modern stroke brain scan technology continues advancing rapidly. Faster MRI sequences reduce scanning time significantly. Artificial intelligence interpretation speeds diagnosis enabling faster treatment decisions.
Mobile stroke units bring imaging directly to patients before hospital arrival. But the fundamental principle remains unchanged regardless of technological advances.
Time is brain when stroke strikes. Every minute without treatment destroys neurons permanently affecting your function.
Understanding when you need emergency stroke brain scan imaging could save your life. It could save the life of someone you love when seconds count.
Don’t hesitate when you see warning signs using FAST or BE FAST assessment. The stroke brain scan you receive in the first hours determines your outcome for years and decades to come after stroke.
Schedule your consultation if you have stroke risk factors requiring preventive evaluation. For emergency stroke symptoms, always call 911 immediately without any delay for emergency stroke brain scan evaluation.